Note: This article was originally posted on November 6, 2020 and was updated and reposted on April 19, 2026.
Introduction
Historically, studies have shown that more than half of weight loss is regained within 2 years, and more than 80% of weight loss is regained by 5 years [1]. Recent data indicate that within 1 year of stopping weekly injections of semaglutide (GLP-1 receptor agonist, 2.4mg), 2/3 of people regain all of their weight [2]. Except for those who regain weight due to a side effect of a newly added medication or a diagnosis of hypothyroidism, why do such a large percentage of people regain most of their lost weight?
Practitioner’s Preface
In my almost 18 years of private clinical practice and my licensure in British Columbia, Alberta, and Ontario have had people come to me with different reasons for seeking my support for weight loss. Some have said their doctor said they were a significant health risk, other times it was because their wife found me and recommended they get help to lose weight, but in my experience, what determines whether they will be successful is where they are in the “Stages of Change”.
What Affects the Outcome?
Some people think that all they need to do is “make up their mind”, but in many cases, people have “made up their minds” multiple times and lost weight, then put it all back again, and more.
Others who have had previous failed attempts at maintaining weight loss often believe that losing weight and keeping it off is a futile endeavour [3], so why bother trying?
Often, it is due to a health concern that people want to change. They know that they need to lose weight to lower their blood sugar or blood pressure, but where to start?
Change is not just a decision. It is a process.
The Stages of Change model was developed in 1979 by James Prochaska [4] and expanded on by Prochaska, Norcross, and DiClemente in their 1994 book Changing for Good [5].
The Stages of Change are Precontemplation, Contemplation, Preparation, Action, Maintenance, and Relapse. Originally viewed as five stages (with Preparation and Action forming one stage), they are now recognized as six distinct stages.
The Six Changes of Change
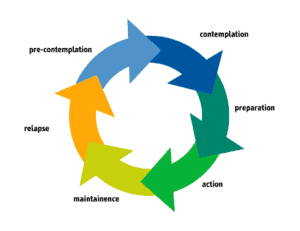
Pre-contemplative – People are beginning to see there is a problem, but not necessarily what it is. Often, they see the problem as outside their control or the result of someone or something else. They may experience negative consequences related to their behaviour, but don’t see the problem as serious enough to motivate change.
Contemplation – The person realizes that their behaviour is problematic, but has mixed feelings. They want the situation to change, but are not ready to commit to making changes.
Preparation – The person still has mixed feelings but begins to make plans to take action within a specific timeframe (usually a few weeks). They weigh the pros (positives) and cons (negatives) and begin creating a plan to support their success.
Action – The person is actively involved in changing their behaviour and carrying out their plan.
Maintenance – People consolidate what they’ve accomplished during the Action stage. They can remain in this stage for extended periods, especially with an adequate support system.
Relapse – The person lapses into former behaviour patterns. Some restart the change process after a brief “slip”, while others continue in their lapsed patterns.
People sometimes come to see me “for a diet” because their doctor or spouse suggested they see a Dietitian. Sure, I could assess them, design a Meal Plan for them and teach them how to implement it, but change is unlikely because they are at the contemplative stage. Their motivation for change is external. While they realize that their eating habits are problematic, they have mixed feelings. They want the situation to change, but are not ready to commit to making changes. On an initial visit, I will try to determine if they have any internal reasons for wanting to change. If they do, and those reasons are important to them, change is possible. If not, I will encourage them to consider why changing how they eat would be valuable to them and to start with services when they are ready.
Other times, people will come to me to help them improve specific health markers, whether it is weight, blood sugar or cholesterol. Their coming to me is their plan to take action, but not actually to change. They are still in the preparation stage. They may actively participate in the assessment process to have a Meal Plan designed for them, but when it comes to learning how to apply it, they are resistant. They may challenge why a food has so many carbohydrates in it, or they may want to know “where chocolate cake fits in my Meal Plan.” These folks may return a few months later, ready to make the changes they were resistant to previously. Sometimes that change is motivated by new lab results, or the ill health of a friend or family member, because, as I refer to it, “change will only occur when the pain of remaining the same is greater than the pain of changing“.
But what about the people who are motivated and successful at accomplishing their goal? Is long-term success guaranteed, or is relapse or “slips” inevitable?
Is Relapse Inevitable?
The standard model views relapse as part of the Stages of Change — and to a certain extent, it is. No one maintains their goal weight, their target blood sugar, or target blood pressure perfectly for an indefinite amount of time.
For some, “relapse” may mean having a meal or dessert that wasn’t part of their plan, but the next day, they get back on track. For others, eating a single meal or dessert triggers feelings of failure, leading to further relapses.
In my experience, two essentials are required for someone to eat off plan, recover and get back on track, versus continuing to relapse.
- The first essential is to lose weight by learning what led to weight gain in the first place, unlearning those behaviours and replacing them with better ones.
A program of protein bar (or protein shake) meal replacements doesn’t teach better eating behaviours. Neither do weekly injections. Weight loss occurs, yes, but when the program or medication is stopped, the weight gain returns. On the other hand, when someone learns improved, sustainable eating behaviours, they understand what ‘eating off plan’ looks like, and they have the tools to make corrections and get back on track.
2. The second essential is having a long-term maintenance plan.
A Long-term Plan for Maintenance
Just as one contemplates a weight-loss plan, prepares to do it, then takes action, long-term success requires a plan not only for losing weight, but also for maintaining it.
I have found that when people understand what contributed to weight gain in the first place, it helps them develop a plan to both lose weight and maintain it.
Each person’s plan will look different. For some, it might involve an accountability partner. For others, it may be support from a Dietitian. For others, dealing with food addiction may find that the support of a 12-step group or an addiction counsellor is invaluable.
Weight loss and weight gain need not be a “vicious cycle.”
Having support from the right people during the process can make all the difference!
If a person is driven to eat by high insulin levels, I help them lower these hormones with simple dietary and lifestyle changes. I often encourage my clients that the issue is “not a weak will, but strong hormones“. A Meal Plan to help them lower high insulin levels enables them to lose weight without always feeling hungry, and to maintain it long-term because they are no longer being “driven” to eat.
If someone realizes that there are certain foods they are absolutely “powerless over”, working with a psychologist to find out if they meet a majority of the criteria for substance use disorder outlined in the Diagnostic and Statistical Manual (DSM), where food is the “abused substance”, can be the first step to getting the help they need. Working with a food addiction counsellor or going to a 12-step group and having me design their Meal Plan that enables them to eat well, while avoiding those “kryptonite foods”, can make it possible.
Some people are driven to “emotional eating“; they eat when they are angry, lonely, tired, or stressed (referred to by the acronym “HALTS”), not because they are hungry. Working with a counsellor to develop alternative behaviours, along with having a Meal Plan that meets their nutritional needs and keeps their blood sugar stable throughout the day, can support long-term success.
“Treatment of obesity requires ongoing attention and support, and weight maintenance-specific counseling, to improve long-term weight management.” [6]
Clinical Application
In my years of clinical experience, the people who came to see me because their doctor or spouse recommended it are rarely successful in losing weight, and on the rare occasion that they are, they rarely sustain the weight loss. That is because the decision was made with an “external locus of control” (outside of themselves). When people make the decision themselves, having worked through the Stages of Change, there is an “internal locus of control”; so people are self-motivated to carry through, and when they have the occasional slip-up.
Final Thoughts…
I support my clients through all the Stages of Change by designing a Meal Plan tailored to their individual needs. Having a clear roadmap that translates their nutrition goals into a sustainable, healthy lifestyle enables them to improve their eating behaviours long-term. When people understand what ‘eating off plan’ looks like, and have the tools to make course corrections, they can get back on track.
I also help clients navigate special occasions where they want to eat off plan without going down the slippery slope of relapse.
I believe that for a change in eating behaviour to be sustainable, unless someone has food addiction, learning to have “sometimes foods” on a special occasion and in what quantity makes that possible. This is the difference between lifestyle changes and a “diet”. If one goes on a diet, they also go off a diet. Learning to navigate real life is what makes change sustainable.
It is entirely possible to be part of the 20% who maintain weight loss at 5 years and beyond by learning sustainable lifestyle changes, with the appropriate support.
More Info
Learn about me and the sustainable weight loss support I provide. View my Comprehensive Dietary Package.
To your good health.
Joy
You can follow me on:
Twitter: https://twitter.com/jyerdile
Facebook: https://www.facebook.com/BetterByDesignNutrition/
References
- Anderson JW, Konz EC, Frederich RC, Wood CL. Long-term weight-loss maintenance: a meta-analysis of US studies. Am J Clin Nutr. 2001;74(5):579–584. [https://pubmed.ncbi.nlm.nih.gov/11684524/]
- Wilding JPH, et al. Weight regain and cardiometabolic effects after withdrawal of semaglutide: The STEP 1 trial extension. Diabetes Obes Metab. 2022 Aug;24(8):1553-1564. [https://pubmed.ncbi.nlm.nih.gov/35441470/]
- Mann T, et al. Medicare’s search for effective obesity treatments: diets are not the answer. Am Psychol. 2007;62(3):220–233. [https://pubmed.ncbi.nlm.nih.gov/17469900/]
- Prochaska JO, DiClemente CC. Transtheoretical therapy: Toward a more integrative model of change. Psychotherapy: Theory, Research & Practice. 1982;19(3):276–288. [https://psycnet.apa.org/record/1984-26566-001]
- Prochaska, J. O., Norcross, J. C., & DiClemente, C. C. (1994). Changing for good. William Morrow and Company.
- Hall KD, Kahan S. Maintenance of Lost Weight and Long-Term Management of Obesity. Med Clin North Am. 2018;102(1):183–197. [https://pubmed.ncbi.nlm.nih.gov/29156185/]

Please note: At this time, all services are provided via a secure telehealth portal.
© 2025 BetterByDesign Nutrition Ltd. All rights reserved.

I am a Registered Dietitian Nutritionist and the owner of BetterByDesign Nutrition Ltd. With a postgraduate degree in Human Nutrition and a background as a published mental health nutrition researcher, I have been dedicated to supporting my clients’ clinical needs since 2008.
I hold active professional licenses in BC (CHPBC), Alberta (CDA), and Ontario (CDO), allowing me to provide regulated Medical Nutrition Therapy across these provinces. My expertise spans chronic disease management, complex digestive health, and therapeutic diets. I am deeply passionate about helping people reclaim their health, rooted in my firm belief that Nutrition is BetterByDesign©.