This article was written on March 22, 2021, and was reviewed and updated by Joy Y. Erdile, MSc, RD, on April 24, 2026.
Practitioner’s Preface
In November 2018, the American Association of Clinical Endocrinologists (AACE) released a Position Statement [1] which identified four separate disease stages associated with an abnormal glucose response, including Type 2 Diabetes:
Stage 1: Insulin Resistance
Stage 2: Prediabetes
Stage 3: Type 2 Diabetes
Stage 4: Vascular Complications — including retinopathy, nephropathy and neuropathy
The Progression of Insulin Resistance
Long before blood sugar becomes abnormal in the stage known as prediabetes, the progression to type 2 diabetes has already begun in the form of insulin resistance — and identifying insulin resistance at this stage (while blood glucose is still normal) enables people to implement dietary changes to avoid the progression to prediabetes and type 2 diabetes.
Discovering insulin resistance in those who lack the more obvious outward signs can be especially helpful — including those who appear slim, but who may have visceral or ectopic fat (so-called TOFIs, “thin on the outside, fat on the inside”), or those who may have undetected hyperinsulinemia due to their abnormal response to dietary carbohydrate. Some people who fall in this category may include those with a significant family history of type 2 diabetes or previous gestational diabetes, even though they currently appear healthy.
What is HOMA-IR?
The Homeostatic Model Assessment (HOMA-IR) is a test that uses a simultaneous fasting blood glucose test and fasting insulin test to accurately estimate the degree of insulin resistance (IR) and β-cell function (the cells of the pancreas that produce insulin). Alternatively, HOMA-IR can also be determined from a simultaneous fasting blood glucose test and a fasting C-peptide test [2]. C-peptide is released in proportion to insulin, so it can be used to estimate insulin.
The HOMA equations have been widely used in research to estimate insulin resistance, and the two equations that use fasting blood levels of insulin and glucose are as follows, with HOMA-IR used to assess insulin resistance and HOMA-B used to assess pancreatic β—cell function [3,9].
HOMA-IR = (glucose in mmol/L x insulin in mIU/mL) / 22.5
HOMA-B = (20 x insulin in mIU/mL) / (glucose in mmol/L – 3.5)
Individual results are best compared to local population cut-off values for HOMA1-IR [3] (1985) or the updated HOMA2-IR [4] (1998).
HOMA2-IR is easily and accurately calculated using the online HOMA2 calculator released by the Diabetes Trials Unit, University of Oxford, available at [http://www.dtu.ox.ac.uk/homacalculator/index.php].
Evolution of the HOMA Model
The original HOMA1-IR equation proposed by Matthews in 1985 [3] was widely used due to its simplicity, it was not always reliable because it did not consider the variations in the glucose resistance of peripheral tissue and liver, or increases in the insulin secretion curve for blood glucose concentrations above 10 mmol/L [5]. The updated HOMA2-IR computer model [6] mentioned above and available from Oxford University corrects for these factors.
Cut-off for insulin resistance using the original Matthews values (1985) [3] for HOMA-IR = 2.7:
- Insulin sensitive: < 1.0
- Healthy: 0.5-1.4
- Early insulin resistance: > 1.8
- Significant insulin resistance: > 2.7
Cut-off values for insulin resistance using the HOMA2-IR calculator (1998) [6] are HOMA2-IR = 1.8. Three population-based studies found the same or very close cut-offs applied, including a 2009 Brazilian study [6] which found HOMA2-IR = 1.8, a 2014 Venezuelan study [7] which found HOMA2-IR = 2.0, and a 2014 Iranian study [8] which found HOMA2-IR = 1.8.
Assessing HOMA-IR and β-cell Function in the Individual
HOMA-IR has been used to assess Insulin Resistance (IR) and β-cell function as a one-off measure in individuals in over 150 epidemiological studies of subjects of various ethnic origins [9]. In the Mexico City Study [10], the development of diabetes was significantly associated with higher HOMA-IR at baseline.
The use of HOMA-IR on an individual basis enables clinicians to quantify both the degree of insulin sensitivity and β-cell function before the person makes any dietary changes. When HOMA-IR is repeated after 6 months of dietary changes, it provides significant feedback regarding effectiveness and motivation to continue.
”HOMA-IR can be used to track changes in insulin sensitivity and β-cell function longitudinally in individuals. The model can also be used in individuals to indicate whether reduced insulin sensitivity or β-cell failure predominates [10].”
Clinical Application
Assessing HOMA2-IR is the reason I will sometimes request a simultaneous fasting blood glucose and fasting insulin blood test for a client. My goal is to find out, even when blood sugar results are still normal, if the pancreas is working too hard to keep them that way.
More Info?
I have several packages that target insulin resistance from different perspectives. For those wanting routine health support for weight management or managing type 2 diabetes or prediabetes, please view the Comprehensive Dietary Package. For women diagnosed with PCOS, please view the Polycystic Ovarian Syndrome (PCOS) Package. You can learn about me here.
To your good health!
Joy
You can follow me on:
Twitter: https://twitter.com/jyerdile
Facebook: https://www.facebook.com/BetterByDesignNutrition/
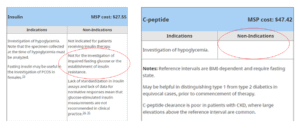
Note: In British Columbia, family MDs may decline to order the fasting insulin test, but a fasting C-peptide test can often be used to determine HOMA2-IR using the Oxford calculator.
References
- American Association of Clinical Endocrinologists. AACE Announces Framework for Dysglycemia-Based Chronic Disease Care Model. November 28, 2018. [https://media.aace.com/press-release/american-association-clinical-endocrinologists-announces-frameworkdysglycemia-based-c]
- Crofts C. Understanding and Diagnosing Hyperinsulinemia. [Doctoral Thesis]. Auckland, New Zealand: AUT University; 2015. p. 205. [https://openrepository.aut.ac.nz/handle/10292/9247]
- Matthews DR, Hosker JP, Rudenski AS, et al. Homeostasis model assessment: insulin resistance and beta-cell function from fasting plasma glucose and insulin concentrations in man. Diabetologia. 1985 Jul;28(7):412-9. [https://pubmed.ncbi.nlm.nih.gov/3899825/]
- Levy JC, Matthews DR, Hermans MP. Correct homeostasis model assessment (HOMA) evaluation uses the computer program. Diabetes Care. 1998 Dec;21(12):2191-2. [https://diabetesjournals.org/care/article/21/12/2191/21431/Correct-Homeostasis-Model-Assessment-HOMA]
- Song YS, Hwang YC, Ahn HY, et al. Comparison of the Usefulness of the Updated Homeostasis Model Assessment (HOMA2) with the Original HOMA1 in the Prediction of Type 2 Diabetes Mellitus in Koreans. Diabetes Metab J. 2016 Aug;40(4):318-25. [https://pmc.ncbi.nlm.nih.gov/articles/PMC4995187/]
- Geloneze B, Vasques AC, Stabe CF, et al. HOMA1-IR and HOMA2-IR indexes in identifying insulin resistance and metabolic syndrome: Brazilian Metabolic Syndrome Study (BRAMS). Arq Bras Endocrinol Metabol. 2009 Mar;53(2):281-7. [https://www.scielo.br/j/abem/a/Fb4KV8mksGnjn9LzfQtQRqR/?lang=en]
- Bermúdez V, Rojas J, Martínez MS, et al. Epidemiologic Behavior and Estimation of an Optimal Cut-Off Point for Homeostasis Model Assessment-2 Insulin Resistance: A Report from a Venezuelan Population. Int Sch Res Notices. 2014 Oct 29;2014:616271. [https://pmc.ncbi.nlm.nih.gov/articles/PMC4897148/]
- Tohidi M, Ghasemi A, Hadaegh F, et al. Age- and sex-specific reference values for fasting serum insulin levels and insulin resistance/sensitivity indices in healthy Iranian adults: Tehran Lipid and Glucose Study. Clin Biochem. 2014 Apr;47(6):432-8. [https://pubmed.ncbi.nlm.nih.gov/24434440/]
- Wallace TM, Levy JC, Matthews DR. Use and Abuse of HOMA Modeling. Diabetes Care. 2004 Jun;27(6):1487-95. [https://diabetesjournals.org/care/article/27/6/1487/25015/Use-and-Abuse-of-HOMA-Modeling]
- Haffner SM, Kennedy E, Gonzalez C, et al. A prospective analysis of the HOMA model: the Mexico City Diabetes Study. Diabetes Care. 1996 Oct;19(10):1138-41. [https://pubmed.ncbi.nlm.nih.gov/8886563/]

© 2025 BetterByDesign Nutrition Ltd.

I am a Registered Dietitian Nutritionist and the owner of BetterByDesign Nutrition Ltd. With a postgraduate degree in Human Nutrition and a background as a published mental health nutrition researcher, I have been dedicated to supporting my clients’ clinical needs since 2008.
I hold active professional licenses in BC (CHPBC), Alberta (CDA), and Ontario (CDO), allowing me to provide regulated Medical Nutrition Therapy across these provinces. My expertise spans chronic disease management, complex digestive health, and therapeutic diets. I am deeply passionate about helping people reclaim their health, rooted in my firm belief that Nutrition is BetterByDesign©.