Note: This article is 6 of 6 articles that have been posted to this website and are in a separate category from research articles, and that category is called “A Dietitian’s Journey”. These 6 articles document my recovery from profound hypothyroidism (June 3, 2022 – October 31, 2022) and represent only my personal experience. They should not be treated as scientific evidence or medical advice.
A Dietitian’s Journey (Part I) documented my personal weight-loss and health-recovery journey (March 5, 2017 – March 4, 2019) and is not posted on this web page.
Introduction
Last Monday, I went to the lab for updated blood work, including a thyroid hormone panel, additional thyroid antibody tests, and an iron panel. I have moved past the frustration of there being no pricelist available for consumers who are self-paying for lab tests, and am now focusing on the lab test results and the dietary changes that I need to make in light of those, as I am recovering from hypothyroidism.
The results came back late Monday afternoon and I met with my doctor to discuss them on Thursday, The good news is that based on calculation estimates converting the bovine Natural Desiccated Thyroid (NDT) medication that I had been taking, to a mixture of Synthroid® (a synthetic T4 medication) and Cytomel® (a synthetic T3 medication), my free T4 and free T3 are almost perfect. As my doctor said when we met, “between your research and my experience, we got this”.
This is a beautiful picture.
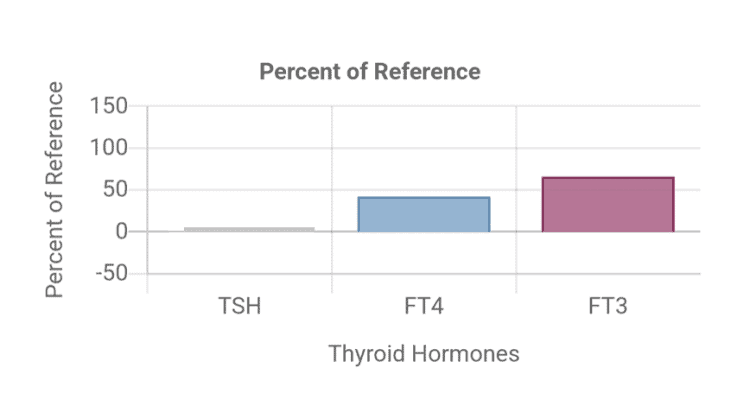
- TSH, fT4 and fT3 levels on T4/T3 thyroid hormone replacement medication
It shows, as my doctor and I had hoped, that my free T3 (the active thyroid hormone) is in the higher part of the reference range (65.5%); a level considered optimal by endocrinologists and thyroidologists who are well-versed in the use of the combination T4/T3 medications that I have been prescribed.
While my free T4 could be in the higher part of the range on the type of medication that I am taking, it may slightly lower because of the feedback from having sufficient free T3. That’s okay! I am feeling so much better, although it will take another year or more until I am really well again.
As expected, my TSH (Thyroid Stimulating Hormone, the pituitary hormone that tells the body how much thyroid hormone to make) is low because the amount of free T3 is optimal. This is a classic feedback loop where free T3 provides feedback on the pituitary gland, indicating that there isn’t a need to make more thyroid hormone. Think of it like a thermostat. When the room gets warm enough, there is feedback on the thermostat that no additional heat is required, and it turns it off until the room gets cold again.
Of importance, my TSH is not considered “suppressed” (TSH ≤0.03 mU/L) but “low” (TSH = 0.04-0.4 mU/liter) [1], so there is no increased risk of cardiovascular disease or bone fractures. Those with a “high” TSH (>4.0 mU/liter) — which was the level that I was at before being treated, and those with a “suppressed” TSH (≤0.03 mU/L) both have an increased risk of cardiovascular disease, abnormal heart rhythms and bone fractures. Those with “low” TSH (0.04-0.4 mU/liter) as I have, do not [1,2]. So more good news.
I have been diagnosed with Hashimoto’s disease (also known as Hashimoto’s thyroiditis), which is an autoimmune disease, and the diagnosis is based on both the symptoms of hypothyroidism, along with the presence of thyroperoxidase antibodies (TPO-ab) and thyroglobulin antibodies (TG-ab) in the blood [3].
In many cases of hypothyroidism, it is these antibodies that contribute to the gradual disappearance of thyroid cells and the development of hypothyroidism. In my case, it was the trauma to the thyroid that resulted from surgery that I had 30 years ago to remove a benign tumour that was the major contributor to the eventual decrease in thyroid function.
Before being diagnosed, as you can read about here, I had all the classic symptoms of hypothyroidism, including body aches, joint pain, fatigue, feeling chilled, constipation, dry skin, hair loss, being forgetful, and even feeling depressed.
By the point I realized that these symptoms were not consistent with long-COVID (which is what I initially suspected) or aging (which my sons assumed), I had developed some of the symptoms of severe hypothyroidism [3], including difficulty with speech, significant water retention, and peripheral edema (swelling) of the ankles and face [3]. There are more photos of what I looked like when I was very sick here, as well as photos from the beginning part of my recovery.
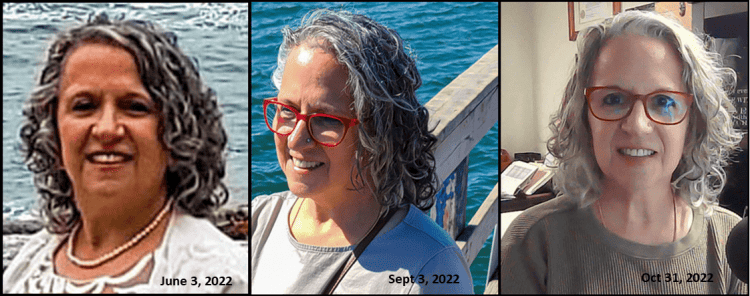
- To hell and back – 5 months of recovery from hypothyroidism
Thyroperoxidase-Ab = 9 (<35 IU/mL)
Thyroglobulin Ab = 14 (<40 IU/mL)
The blood tests indicated that while I have some thyroperoxidase antibodies (TPO-Ab) and thyroglobulin antibodies (TG-Ab), I do not have Hashimoto’s disease (autoimmune) as neither was over the lab cutoffs.
As diagnosed by my doctor based on previous lab results and symptoms, I have hypothyroidism, but based on this lab work, it is not autoimmune in nature.
Gliadin and Transglutaminase
For many years, I avoided gluten-containing products because I thought I was gluten-intolerant, although not celiac.
A year ago, I stumbled across some novel ingredients and had an idea to create low-carb breads to provide dietary options for those with diabetes. My goal was to enable people who would not otherwise consider a low-carbohydrate diet to be able to adopt one, for health reasons. I was mainly thinking of those from bread-centric cultures, such as South East Asians (Indian) and Hispanics, but in time, I developed many more types of low-carb bread.
I was aware of the connection between high gluten consumption and leaky gut syndrome, but against that, I weighed the serious morbidity and mortality linked to uncontrolled diabetes. I had come across many people who would rather stay diabetic, and potentially lose their toes or vision, than give up bread and developing these breads seemed like the lesser of two evils.
Since being diagnosed with hypothyroidism, which I had been developing over the previous 9 years (more about that here), I learned that the gliadin fraction of gluten structurally resembles transglutaminase. Transglutaminase is an enzyme that makes chemical bonds in the body, and while present in many organs, there are higher concentrations of transglutaminase in the thyroid.
In leaky gut syndrome, gliadin (and other substances) result in the gaps in between the cells of the intestinal wall widening. This results in the immune system of the body reacting to food particles that are inside the intestine, which it normally would not see. It is thought that the immune system reacts to gliadin and creates antibodies to it, seeing it as a foreign invader. Since gliadin and transglutaminase have very similar structural properties, it is thought that in those with leaky gut syndrome, the immune system begins to attack the transglutaminase in the thyroid and other tissues, contributing to the development of autoimmune conditions, including Hashimoto’s.
A-1 Beta Casein and Gluten
A few years ago, I had leaky gut syndrome but it resolved with dietary changes, including avoiding gluten and A-1 beta casein dairy (you can read about what A-1 beta casein dairy is here). Naturally, as I had been working on recipe development for the low-carb bread book, I had been eating gluten as I tested them. I also became more liberal in including dairy products from A1-beta casein cows, when I hadn’t used them in years. That started when there was severe flooding last year in Chilliwack last year due to heavy rains after the summer, and that was where my goat milk came from. Even once the roads were open again and the highways rebuilt, I never really went back to using goat milk, which is naturally A-2 beta casein. In the interest of an abundance of caution, I will go back to using dairy products from A-2 beta casein cows, or from goat or sheep milk (that are naturally A-2). Humans produce A-2 beta casein protein, and using milk from A-2 beta casein animals does not result in an immune response. It is not seen as “foreign.”
From what I’ve read and in discussing it with my doctor, it is likely that my hypothyroidism has been developing over the last 30 years, related to the surgery I had to remove a benign tumour. Further supporting that my becoming hypothyroid has been a long time in the making, I have had high-normal levels of TSH over the last 9 years — which happens to be a time period over which I was avoiding both gluten and A-1 dairy. Given that, I think it’s logical to conclude that my hypothyroidism is primarily related to the destruction of thyroid tissue in the invasive surgery connected to the removal of the tumour. Further supporting this hypothesis, I currently have fairly low levels of TPO and TG antibodies, so I suspect they have begun developing fairly recently. Since a 2018 study reported that both TPO-antibodies and TG-antibodies are decreased in hypothyroid patients following a gluten-free diet [4], it seems wise for me to go back to avoiding gluten, to lower my TPO-antibodies and TG-antibodies as close to zero as possible.
Cruciferous Vegetables
Cruciferous vegetables such as Brussels sprouts, broccoli, bok choy, cauliflower, cabbage, and kale are known as goitrogens. Goitrogens are naturally occurring substances that are thought to inhibit thyroid hormone production. The hydrolysis of a substance known as pro-goitrin that is found in cruciferous vegetables produces a substance known as goitrin, which is thought to interfere with thyroid hormone synthesis [5]. Since cooking cruciferous vegetables limits the effect on the thyroid function, and eating cruciferous vegetables has many health benefits, I will usually eat them cooked, but not in huge quantities. Some studies found a worsening of hypothyroidism when people ate very large quantities of these (e.g. 1 – 1 ½ kg / day) so it is recommended that intake of these vegetables be kept relatively constant day to day, and limited to no more than 1-2 cup/day. I’ve decided that when I do eat them, to keep intake to the lower end of that range and eat more non-cruciferous vegetables instead.
Iron Deficiency and Low Stomach Acid (hypochlorhydria)
I now know why I am still so tired. I asked my doctor to run an iron panel, and the results show I have low iron. Previous results indicate my vitamin B12 are fine, and I continue to supplement methylated folate and B12, so I know those are not a problem.
While my iron stores (ferritin) are okay, they are not optimal, i.e., ferritin = 93 (15-247 ug/L) instead of >100ug/L.
My hematology panel is low-normal i.e. hemoglobin = 122 (115-155 g/L), hematocrit = 0.37* (0.35-0.45 L/L), MCV = 88 (82-98 fl), MCH = 29.5 (27.5-33.5 pg), MCHC = 334 (300-370 g/L)
My serum iron and iron saturation are very low, i.e., serum iron = 11.9 (10.6-33.8 umol/L), iron saturation = 0.15 (0.13-0.50)
Low iron status is common with hypothyroidism, but it was surprising to me because I eat beef liver, or chicken livers every week, and also take a heme polysaccharide supplement (like Feramax®), so it may be due to an absorption problem.
Low stomach acid (hypochlorhydria) is common in hypothyroidism, and since low pH is needed for iron absorption, I have made dietary changes to improve that.
Final Thoughts…
I am very grateful that my doctor recognizes my knowledge as a clinician and is receptive to me advocating for my health. I am incredibly fortunate that he involves me in decisions regarding blood tests, as well as discussing medication types and dosages. As for the dietary changes and supplementation, he is content to let me handle that!
I hope that out of my experience, which I have called “to hell and back” I can help others better understand hypothyroid symptoms, diagnosis and treatment options so that they can discuss them with their doctor.
To your good health,
Joy
Copyright ©2022 BetterByDesign Nutrition Ltd.
LEGAL NOTICE: The contents of this blog, including text, images and cited statistics as well as all other material contained here (the ”content”) are for information purposes only. The content is not intended to be a substitute for professional advice, medical diagnosis and/or treatment and is not suitable for self-administration without the knowledge of your physician and regular monitoring by your physician. Do not disregard medical advice and always consult your physician with any questions you may have regarding a medical condition or before implementing anything you have read or heard in our content.

I am a Registered Dietitian Nutritionist and the owner of BetterByDesign Nutrition Ltd. With a postgraduate degree in Human Nutrition and a background as a published mental health nutrition researcher, I have been dedicated to supporting my clients’ clinical needs since 2008.
I hold active professional licenses in BC (CHPBC), Alberta (CDA), and Ontario (CDO), allowing me to provide regulated Medical Nutrition Therapy across these provinces. My expertise spans chronic disease management, complex digestive health, and therapeutic diets. I am deeply passionate about helping people reclaim their health, rooted in my firm belief that Nutrition is BetterByDesign©.