Introduction
NOTE: This article contains aspects of my personal story which are clearly marked. My personal experience is not objective data. The pictures are provided only so that people can better understand what the “weight gain” of hypothyroidism can look like, and how different it is from ordinary weight gain.
In-person visits to the doctor have been minimal over the past two years, and it has been easy for people to discount symptoms such as body aches, headaches, fatigue, and ‘brain fog’ as having had Covid, or to having ‘long Covid’ [1]. It was only when I began having symptoms that were not consistent with COVID that I began to think that it might be hypothyroidism.
I am not that old, but at the beginning of June (two months ago), our family was in Tofino (Vancouver Island) for the marriage of my youngest son. The groom’s eldest brother assumed that my inability to walk on the sand, up the path to the hotel, or get up from a chair was a result of my having “aged.”
 He had no idea that I was hiking in North Vancouver and Golden Ears Provincial Park for several hours at a time last summer. I knew that it was abnormal for me to feel so exhausted and for my muscles to feel so weak, and one look in the mirror told me something was very wrong.
He had no idea that I was hiking in North Vancouver and Golden Ears Provincial Park for several hours at a time last summer. I knew that it was abnormal for me to feel so exhausted and for my muscles to feel so weak, and one look in the mirror told me something was very wrong.
In a matter of just a few weeks, I went from looking as I have for the last two years to looking as I did when I was 55 pounds overweight. For the sake of this special occasion, I said nothing to my family, but I was very concerned for my health. It was also exceedingly hard for me to be in family photographs that I knew would be viewed for years to come.
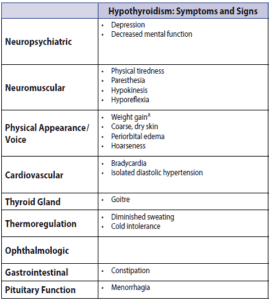
Common Hypothyroid Symptoms and the Aging Myth
-
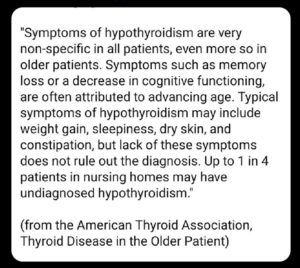
from https://www.thyroid.org/thyroid-disease-older-patient/
People assume that it is normal for ‘older adults’ to have body aches, joint pain, fatigue, feel chilled when others do not, experience constipation, have dry skin or hair loss, be forgetful, or even experience depression. However, these are NOT typical signs of aging but ARE common symptoms of hypothyroidism.
Consider constipation as an example. Chronic constipation affects 15% of adults and is the sixth most commonly reported GI symptom [3]. Within the context of a lack of mobility that we have all faced due to lockdown restrictions, how many people would give increased constipation a second thought?
Untreated Hypothyroidism and Myxedema
Myxedema describes advanced hypothyroidism that occurs when the condition is left untreated or inadequately treated [4]. This term is also applied to hypothyroidism’s effects on the skin, where it looks puffy and swollen and takes on a waxy consistency [4].
Myxedema of hypothyroidism is very different from ordinary weight gain. I hope that by sharing these photos, people will be better equipped to recognize this symptom in themselves or in others, and ensure that medical attention is sought.
The Challenges of Getting Diagnosed
In British Columbia, thyroid testing covered by the provincial health plan is determined by a 2018 document titled Thyroid Function Testing in the Diagnosis and Monitoring of Thyroid Function Disorder [2]. These guidelines outline testing for thyroid-stimulating hormone (TSH), free thyroxine (fT4), free triiodothyronine (fT3), and anti-thyroid peroxidase (TPO).
The problem is that typical symptoms such as cold intolerance, edema, decreased sweating, and skin changes often don’t appear until much later in the progression of the disease.
NOTE: These photos are for illustrative purposes only.
[LEFT: me hiking March 5, 2022. MIDDLE: me at my youngest son’s wedding at the beginning of June, 2022. RIGHT: Me today (August 8, 2022), with 75% of the edema resolved.]

UPDATE [August 25, 2022]: The photo on the left was taken 2 ¾ months ago. The photo on the right was taken today, 2 months after beginning treatment for hypothyroidism.
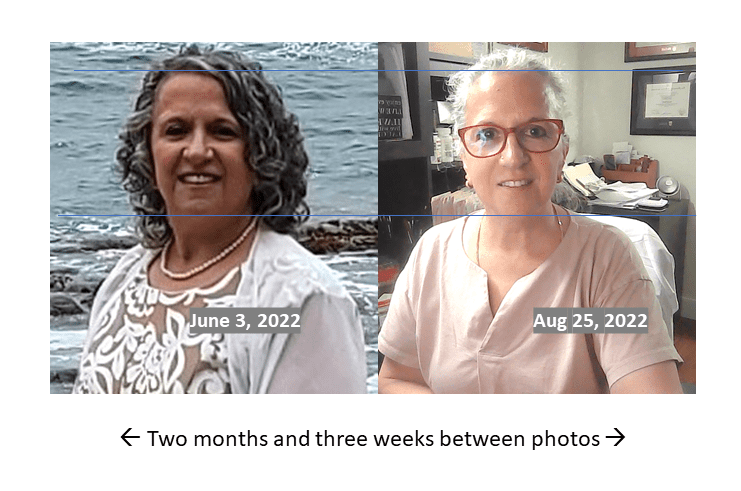

While each person may exhibit different symptoms, this is fairly typical of the length of time over which the “weight gain” of hypothyroidism can occur, and also the time frame over which it can resolve with treatment.
The Danger of Myxedema Crisis
It is important to understand that untreated hypothyroidism can progress to a myxedema crisis, which can be fatal. The death rate for a myxedema crisis is between 20-60%, even with treatment [5].
The most noticeable feature of a myxedema crisis is the person’s significant deterioration in mental function [5]. In severe untreated hypothyroidism, people can exhibit significant agitation and even psychosis and paranoia, referred to as “myxedema madness” [6].
Final Thoughts…
By virtue of their age, older adults in British Columbia qualify for thyroid testing. If older people exhibit even a few of the common symptoms of hypothyroidism, this should be brought to their doctor’s attention.
In British Columbia, someone can pay (at government rates) $9.90 for a TSH test, $12.12 for a free T4 test, and $9.35 for a free T3 test [9]. Licensing requirements require doctors who write a lab test requisition to also take responsibility for overseeing care based on those results. Unfortunately, not all doctors are willing to treat those with subclinical hypothyroidism.
More Info
As you can read about under the About Me tab, I will advocate for clients who have symptoms that may be consistent with hypothyroidism or subclinical hypothyroidism to obtain adequate testing to rule out a diagnosis or enable a doctor to make one. You can view the Hypothyroid Management Package here.
To your good health!
Joy
You can follow me on:
Twitter: https://twitter.com/jyerdile
Facebook: https://www.facebook.com/BetterByDesignNutrition/
Quick Clinical Summary
Q: Are body aches and fatigue just a normal part of aging?
A: No. While often dismissed as signs of getting older, symptoms like chronic joint pain, extreme fatigue, forgetfulness, and cold intolerance are hallmark signs of hypothyroidism and should be evaluated by a physician.
Q: What is myxedema and how does it affect appearance?
A: Myxedema is a clinical term for advanced, untreated hypothyroidism. It causes the skin to appear puffy, swollen, and waxy due to the accumulation of mucin. This can cause a rapid change in appearance that mimics significant weight gain.
Q: What is ‘Myxedema Madness’?
A: In severe, untreated cases of hypothyroidism, a person can experience a significant deterioration in mental function, including agitation, paranoia, and psychosis. This clinical state is historically referred to as ‘myxedema madness’.
References
- Johns Hopkins Medicine. Long COVID: Long-Term Effects of COVID-19. [Published 2022 Jun 14]. [https://www.hopkinsmedicine.org/health/conditions-and-diseases/coronavirus/covid-long-haulers-long-term-effects-of-covid19]
- BC Guidelines & Protocols Advisory Committee. Thyroid Function Testing in the Diagnosis and Monitoring of Thyroid Function Disorder. Victoria (BC): Ministry of Health; 2018 Oct 24. [https://www2.gov.bc.ca/gov/content/health/practitioner-professional-resources/bc-guidelines/thyroid-function-testing]
- Bharucha AE, Lacy BE. Mechanisms, Evaluation, and Management of Chronic Constipation. Gastroenterology. 2020 Apr; 158(5):1232-1249.e3. [https://doi.org/10.1053/j.gastro.2019.12.034]
- Medical News Today. What is Myxedema and How is it Treated? [Updated 2022 Apr 22]. [https://www.medicalnewstoday.com/articles/321886]
- Elshimy G, Chippa V, Correa R. Myxedema. [Updated 2022 May 22]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing. [https://www.ncbi.nlm.nih.gov/books/NBK545193/]
- Samuels MH. Psychiatric and cognitive manifestations of hypothyroidism. Current Opinion in Endocrinology, Diabetes and Obesity. 2014 Oct; 21(5):377-383. [https://doi.org/10.1097/MED.0000000000000089]
- Heinrich TW, Grahm G. Hypothyroidism Presenting as Psychosis: Myxedema Madness Revisited. Primary Care Companion to the Journal of Clinical Psychiatry. 2003; 5(6):260-266. [https://doi.org/10.4088/pcc.v05n0603]
- Patil N, Rehman A, Jialal I. Hypothyroidism. [Updated 2022 Jun 19]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing. [https://www.ncbi.nlm.nih.gov/books/NBK519536/]
- Government of British Columbia, Ministry of Health. Schedule of Fees for Laboratory Services – Outpatient, Payment Schedule. [Revised 2022 Apr 1]. [https://www2.gov.bc.ca/assets/gov/health/practitioner-pro/medical-services-plan/laboratory_services_schedule_of_fees.pdf]
- BC Agency for Pathology and Laboratory Medicine (BCAPLM). Outpatient Payment Schedule, Laboratory Volume Discounting (LVD). [Accessed 2022 Aug 14]. [https://www2.gov.bc.ca/gov/content/health/practitioner-professional-resources/msp/registers-manuals-and-reports/laboratory-services-outpatient-payment-schedule]

© 2025 BetterByDesign Nutrition Ltd. All rights reserved.

I am a Registered Dietitian Nutritionist and the owner of BetterByDesign Nutrition Ltd. With a postgraduate degree in Human Nutrition and a background as a published mental health nutrition researcher, I have been dedicated to supporting my clients’ clinical needs since 2008.
I hold active professional licenses in BC (CHPBC), Alberta (CDA), and Ontario (CDO), allowing me to provide regulated Medical Nutrition Therapy across these provinces. My expertise spans chronic disease management, complex digestive health, and therapeutic diets. I am deeply passionate about helping people reclaim their health, rooted in my firm belief that Nutrition is BetterByDesign©.